June 23, 2019
Where you call home determines how long you live
A few miles can add up to years when it comes to life expectancy
~
BY Brian Conway
Across America, life expectancy varies drastically between communities separated by a handful of miles.
In Chicago’s South Side, people from Washington Park live, on average, 16 fewer years than people living in The Loop, downtown, eight subway stops away.
In Detroit, residents of Grosse Pointe can expect to live until about 82; a few miles away, in Midtown, the life expectancy is 69.
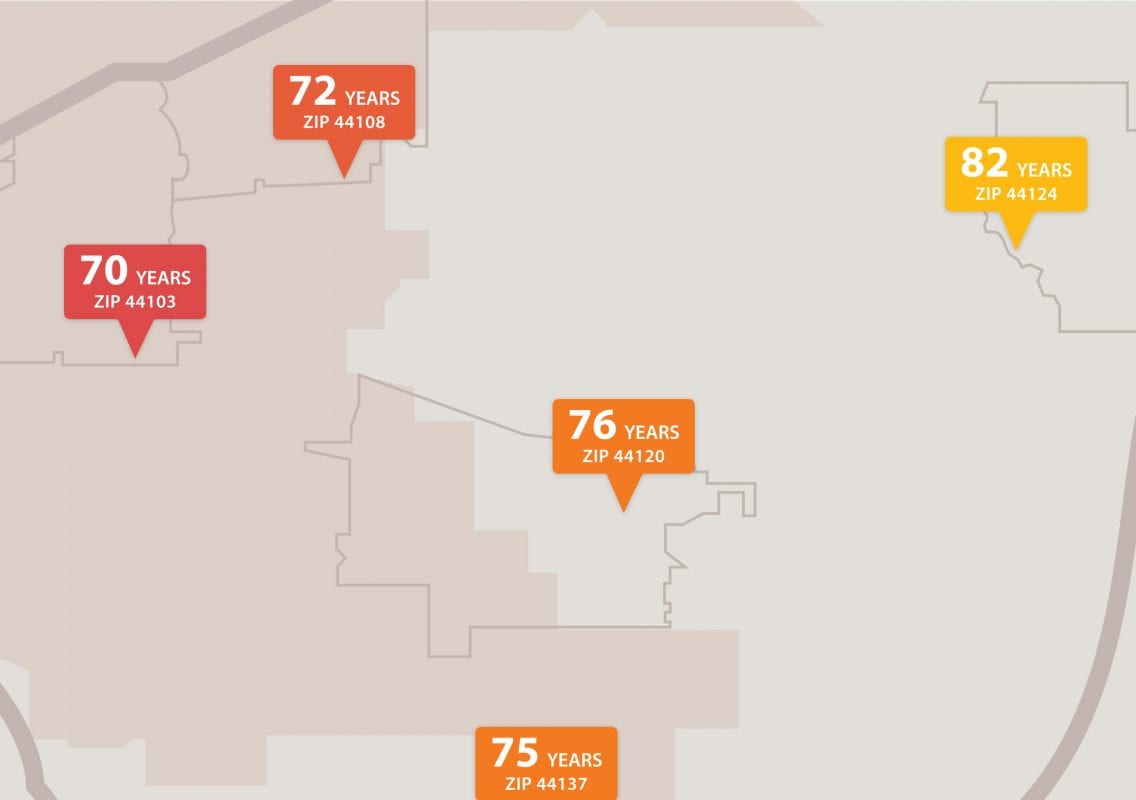
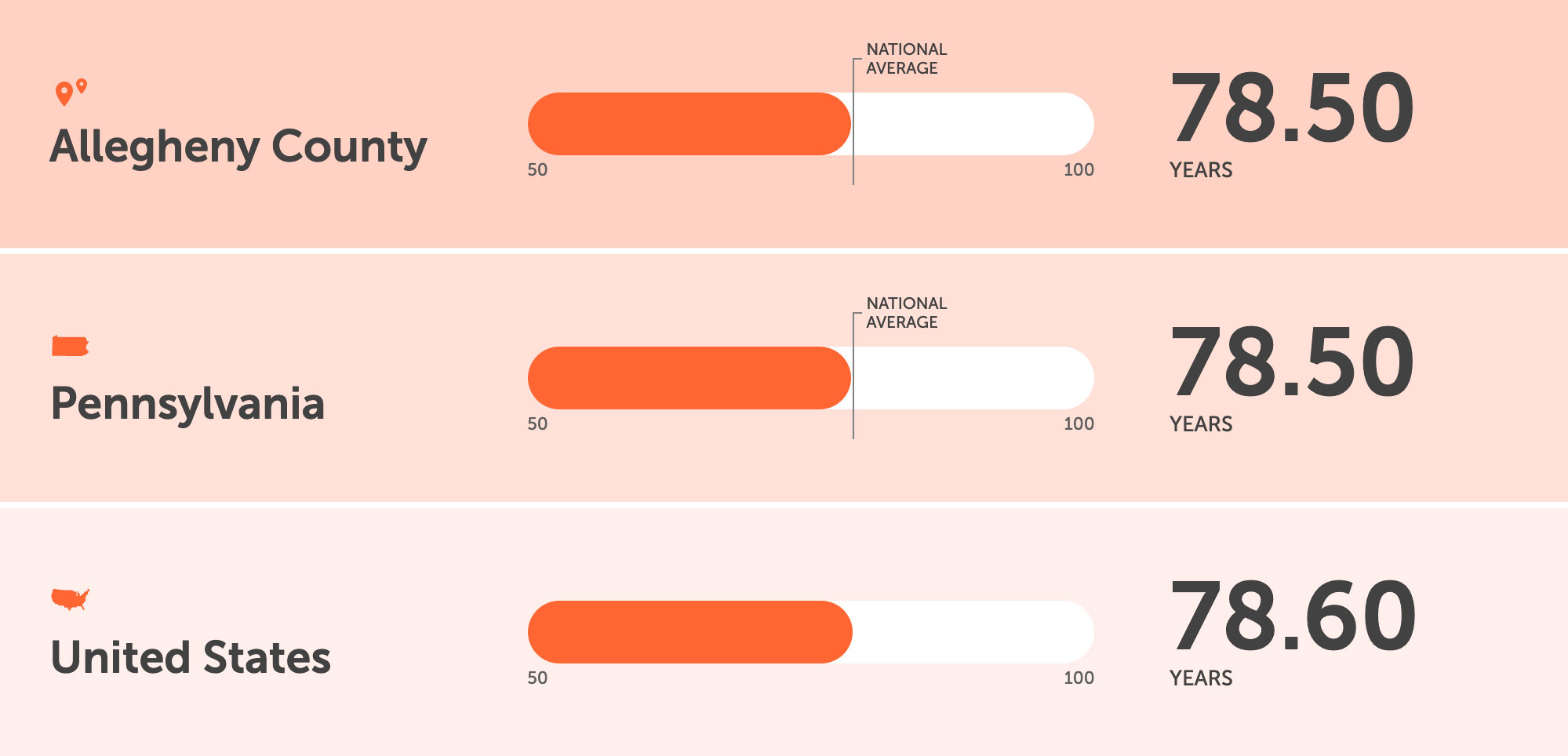
In Pittsburgh, it’s no different. In parts of the historically black Hill District, it’s 69.6 years. In gentrified Upper Lawrenceville, 79.4. In Clairton, a city some 10 miles south and home to the nation’s largest coke manufacturing facility: 73.5. The national average is 78.6.
“In our society, we’ve created neighborhoods particularly built along people’s socioeconomic status,” said Kenneth Thompson, a Pittsburgh-based psychiatrist and researcher. “And the socioeconomic status that you have is probably the predominant driver, of a whole community of people, of the average health and the length of life of the population that live there.”
To address inequity at home, government and nonprofit officials in Pittsburgh have entered into a partnership with the city of Glasgow, Scotland, a similarly placed postindustrial city known to fall under the “the sick man of Europe” label due to its poor health outcomes. But Glasgow has made notable improvements in certain mortality rates in recent years, and Pittsburgh officials hope to emulate its turnaround.
“We see a high rate of disease along our rivers, along where there had been industrial production years and years ago that is now gone, but the waste and the byproducts have infected the soil and the air that these individuals breathe,” said Lou Ann Jeremko, executive director of Pittsburgh’s Consumer Health Coalition and co-investigator in the Glasgow partnership.
She stresses they don’t know causality, only that people who live in such areas are dying at a younger age and show higher rates of chronic disease, ranging from asthma to cancer.
“Those are what we call inequities,” she said. “Individuals in a city [filled] with wonderful, quality healthcare providers, but not always having the same access, awareness, and knowledge.”
~
“We see a high rate of disease along our rivers, along where there had been industrial production years and years ago that is now gone, but the waste and the byproducts have infected the soil and the air that these individuals breathe.”
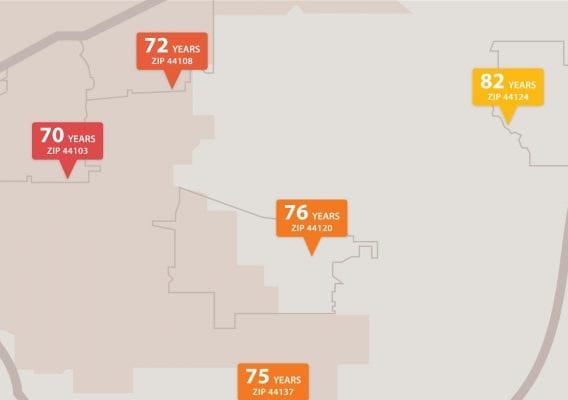
Sourced from, Could where you live influence how long you live? Put in your address and see how you compare.
Thompson, who puts forth a social-ecological view of health and wellness, notes that while of course genetics and behavior and other factors play a role in health, populations in the same area shouldn’t have average life expectancies that differ by decades.
“How we experience both illness and well-being are heavily influenced by what happens between us and how we organize and make our world,” Thompson said.
In the 90s, Thompson received a grant from the Soros Foundation to become a physician advocate fellow in the United Kingdom, where he focused on health in former industrial cities, including Glasgow, making him an ideal co-principal, alongside Jeremko, for the Pittsburgh-Glasgow partnership.
Funded by the Robert Wood Johnson Foundation, the nation’s largest philanthropy for public health, the grant connects Pittsburgh institutions with Resilient Glasgow and the Glasgow Centre for Population Health so that Pittsburgh can begin to establish a “culture of health.”
A culture of health “is really taking a very holistic perspective to what is needed to achieve health and well-being,” including food, transportation, jobs, and many other factors, said Karabi Acharya, a director with the RWJF.
Both Glasgow and Pittsburgh are part of the 100 Resilient Cities network, a global resiliency initiative sponsored by the Rockefeller Foundation.
“We understood that, looking at both cities’ strategies, that we have a lot of common confluences, both of which begin with the fact that we are those postindustrial cities,” City of Pittsburgh Chief Resilience Officer Grant Ervin said.
Ervin said that Glasgow and Pittsburgh are pursuing a potential sister city relationship, which would allow for further collaboration in the future.
Of particular concern in both cities is the rise of “diseases of despair” — deaths caused by opiates, suicide, and alcohol. Today, Thompson said mortality rates are increasing among poor, undereducated white men and women, particularly men in their 30-60s. “They’re dying younger than they were before, and this is the first time we’ve seen this happen in American history that we’ve kept any meaningful data.”
Thompson said these illnesses come about when a population gives up on some fundamental sense of hope or notion of future opportunity, as was witnessed in present-day Russia around the collapse of the Soviet Union.
“The more opportunities that you have, the healthier you are likely to be,” Thompson said, “and the healthier you are, the more likely you are to have opportunities.”
~
“How we experience both illness and well-being are heavily influenced by what happens between us and how we organize and make our world.”
Pete Seaman, acting associate director at the Glasgow Centre for Population Health, said that traditional medical services are not well-suited to manage conditions that are psycho-social in origin, such as anxiety or depression, nor are they set up to deal with the behaviors that stem from them, such as substance use.
Chronic liver disease, lung cancer, deaths from suicides, overdoses, and violence are rising in Scotland, Seaman said, something that highlights the limits of a modernist model of medicine and public health.
“To tackle these we need to change the conditions in which people live, so they can live meaningful lives,” he said in an email.
But remedying health inequity requires confronting unpleasant, unresolved truths, as well as big-picture questions about how society is organized.
“How do you find the investment, how do you create the political will to actually make places healthy and well?” Thompson asked. “That’s clearly biggest challenge.
“At the larger level, what we are really trying to figure out is how to leverage both politically and economically the role of reinvestment into communities and people.”
In many sectors, a consensus is emerging that systemic change must be implemented to achieve health equity, or, at the very least, modifications must be made to how existing systems interact with one another.
It’s a sentiment echoed by Karen Hacker, the head of the Allegheny County Health Department.
“We have to work with a lot of sectors,” she said. “The health department is not in charge of housing. The health department is not in charge of transportation. But what we’ve been trying to do is work cross-sector to convene people to basically help them focus on some of these communities that are really suffering in many ways.”
In Allegheny County, as with most everywhere, equity is not being achieved, and there’s a direct correlation between poverty and negative health outcomes, Hacker noted.
“If you look at all the data,” she said, “what you’ll see is that almost every indicator from our behavioral risk factor survey is that the eastern side of our county is experiencing more negative health outcomes than the western side, and you see that over and over again, whether it’s diabetes, or hypertension, or asthma, again, many of these things are absolutely connected with levels of poverty.”
Hacker said that health equity has been a particular concern for her department in recent years, and the data it assembles on inequities is used to govern its interventions. On the health department’s website, residents can access community indicators to compare their neighborhood with other local, state, and national data regarding access to care, chronic disease behaviors, mental health, maternal health, and the environment.
For now, Thompson said there’s no cheap or immediate solution that would make a significant impact in health equity in Pittsburgh, but he believes that a helpful first step would be improving primary health services in a way that made them more linked to community resources.
“We have a very underdeveloped primary health network in Allegheny County,” Thompson said, “and our health services at the primary health level are not very engaged with our communities, particularly in the communities that are most struggling.”

Brian Conway is a freelance reporter based in Pittsburgh. His investigations into the city's lead in water crisis earned him First Prize for Environmental Reporting from the Keystone Chapter of the Society for Professional Journalists in their statewide Spotlight contest. In addition to investigative and enterprise reporting, he also covers Pittsburgh's music, craft beer, and cannabis scenes for a variety of publications, and is a member of the Work Hard Pittsburgh digital media cooperative. Follow him on Twitter and Instagram.
~
Share this page